Chronic Exertional Compartment Syndrome
What is Chronic Exertional Compartment Syndrome?
Chronic exertional compartment syndrome (CECS) is a cause of exercised-induced leg and foot pain.
- Chronic - present for some time, not acute (which is a surgical emergency).
- Exertional - caused by exercise.
- Compartment syndrome - swelling causing increased pressure inside a fixed volume (compartment) of the body.
The muscles in the leg are grouped into compartments surrounded by deep fascia, a layer of inflexible fibrous tissue under the skin and between the bones.
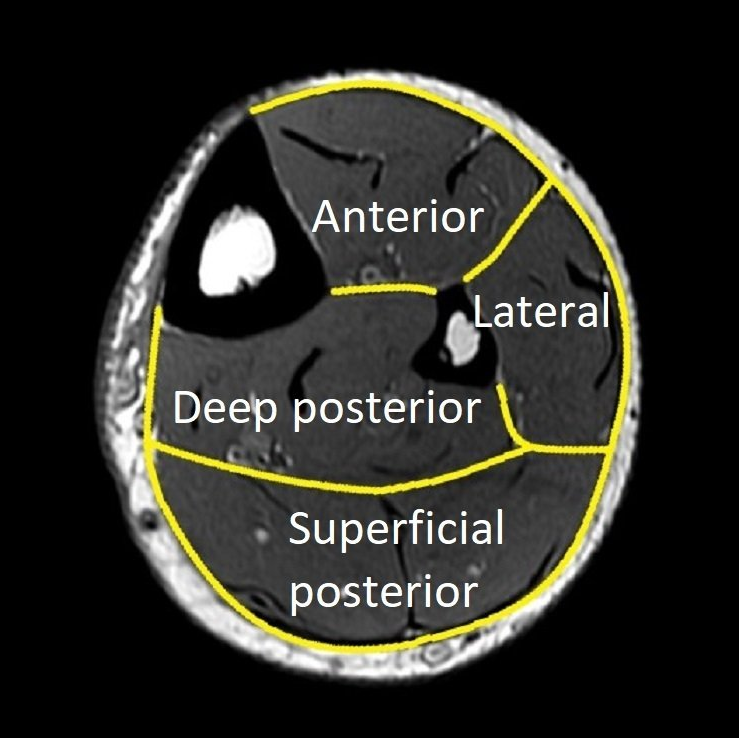
There are four compartments in the leg (please see images below):
- anterior (front of shin)
- lateral (outer leg)
- superficial posterior (calf muscles)
- deep posterior (deep leg).
Chronic exertional compartment syndrome usually involves the anterior and/or lateral compartments of the leg. It can also occur in the inner foot.

Other Causes of Exercise-induced Leg Pain
Other causes of exercised-induced leg pain include:
- medial tibial stress and "shin-splints" (common)
- anterior tibial stress fracture (uncommon but important)
- "fascial" hernia
- superficial peroneal nerve hiatus compression
- popliteal artery entrapment syndrome (rare, usually one calf only).
With aging, other causes of leg pain become more common:
- tendinopathy
- arthritis
- spinal stenosis
- peripheral vascular disease.
Causes of Chronic Exertional Compartment Syndrome
- age less than 30 years
- running
- over-training.
Chronic Exertional Compartment Syndrome Symptoms
- cramping/burning bilateral leg pain which:
- recurs every time a certain level of exercise is achieved (duration, intensity, distance, etc)
- get worse with continued exercise
- gets better with rest
- mild leg weakness and sensation changes until rest occurs.
Chronic Exertional Compartment Syndrome Diagnosis
The diagnosis of CECS is made by taking a complete history and performing a physical examination.
Keys to diagnosis are :
- pain is only with exercise and improves with rest (see risk factors and symptoms above)
- the shin bone (tibia) is not tender or swollen
- pulses and nerve function are normal at rest.
Imaging has a limited role :
- X-rays are often preformed (usually normal)
- bone scan is used to rule out medial tibial stress and anterior tibial stress fracture (usually not needed)
- pre and post-exercise MRI can show muscle compartment oedema (expensive and experimental)
- ultrasound can assess for "fascial" hernias, nerve compression and popliteal artery entrapment.
Intra-compartmental pressure monitoring :
- can be used to confirm the diagnosis using the Modified Pedowitz Criteria
- requires a needle inserted into the various compartments
- requires pressure measurement before and after (+/- during) exercise
- is available in Adelaide (Dr Duncan Walker).
CECS is a clinical diagnosis . Not all cases require imaging or pressure monitoring.





Chronic Exertional Compartment Syndrome Treatment
Non-surgical treatment
Surgical treatment
Surgery for CECS involves increasing the size of the affected compartment(s) by fasciotomy.
The anterior and/or lateral compartments are released through two incisions along the outer leg. This protects the nerves from injury and allow full release without a single long scar. If needed, the posterior compartments can be released though a medial incision.
Release of the anterior and/or lateral compartments relieves CECS pain by three months in 80% of people.
People requiring posterior compartment release take longer to recover and only 65% are significantly better.
Both legs can have surgery at the same time.
Dr Beamond may arrange for an ultrasound on the morning of surgery to locate the superficial peroneal nerve. This can reduce scar length and improves safety.
Surgery:
- is Day Surgery (unless all compartment in both legs)
- requires a general anaesthetic
- takes 30 minutes per leg.
First 2 weeks:
- compression bandage(s)
- weight bearing +/- crutches
- rest, elevation and ice (RICE)
- ankle and toe movements
- post-operative appointment.
Next 2 months:
- RICE as needed
- physiotherapy-guided stretching
- exercise bike, pool and gym exercises
- return to sports specific training.
Benefits and risks:
- 65 - 80% of people are helped by surgery
- 20 - 35% of people are not helped by surgery
- 5% of people are made worse by surgery.
Consequences and complications:
- driving restrictions (2 to 4 weeks)
- muscle "bulging" can occur
- scar numbness is common
- major nerve injury is uncommon
- see General Information about Surgery .